As such, the correct next step for addressing her floppy eyelids wasn’t eye surgery or medication—it was a referral for a sleep test.
The patient did the test, which found that while she was sleeping, she stopped breathing 27 times per hour. On the apnea–hypopnea index, that yields a diagnosis of moderate-level OSA.
With this finding, the woman started using a continuous positive airway pressure (CPAP) machine, which delivers continuous air into the airway during sleep, preventing it from closing up. Along with some eye lubricants, nighttime eye patches, and a weight-loss plan, the woman’s condition rapidly improved. After two weeks, her eyelids were no longer inside out, and she could properly close her eyes. She was also sleeping better and no longer had daytime drowsiness.
Doctors don’t entirely understand the underlying mechanisms that cause floppy eyelid syndrome, and not all cases are linked to OSA. Researchers have hypothesized that genetic predispositions or anatomical anomalies may contribute to the condition. Some studies have found links to underlying connective tissue disorders. Tissue studies have clearly pointed to decreased amounts or abnormalities in the elastin fibers of the tarsal plate, the dense connective tissue in the eyelids.
For people with OSA, researchers speculate that the sleep disorder leads to hypoxic conditions (a lack of oxygen) in their tissue. This, in turn, could increase oxidative stress and reactive oxygen species in the tissue, which can spur the production of enzymes that break down elastin in the eyelid. Thus, the eyelids become lax and limp, allowing them to get into weird positions (such as inside out) and leading to chronic irritation of the eye surface.
The good news is that most people with floppy eye syndrome can manage the condition with conservative measures, such as CPAP for those with OSA, as did the woman in New York. But some may end up needing corrective surgery.
The man made a full recovery, but this tale is not for the faint of heart.
If you were looking for some motivation to follow your doctor’s advice or remember to take your medicine, look no further than this grisly tale.
A 64-year-old man went to the emergency department of Brigham and Women’s Hospital in Boston with a painful festering ulcer spreading on his left, very swollen ankle. It was a gruesome sight; the open sore was about 8 by 5 centimeters (about 3 by 2 inches) and was rimmed by black, ashen, and dark purple tissue. Inside, it oozed with streaks and fringes of yellow pus around pink and red inflamed flesh. It was 2 cm deep (nearly an inch). And it smelled.
The man told doctors it had all started two years prior, when dark, itchy lesions appeared in the area on his ankle—the doctors noted that there were multiple patches of these lesions on both his legs. But about five months before his visit to the emergency department, one of the lesions on his left ankle had progressed to an ulcer. It was circular, red, tender, and deep. He sought treatment and was prescribed antibiotics, which he took. But they didn’t help.
You can view pictures of the ulcer and its progression here, but be warned, it is graphic. (Panel A shows the ulcer five months prior to the emergency department visit. Panel B shows the ulcer one month prior. Panel C shows the wound on the day of presentation at the emergency department. Panel D shows the area three months after hospital discharge.)
Gory riddle
The ulcer grew. In fact, it seemed as though his leg was caving in as the flesh around it began rotting away. A month before the emergency room visit, the ulcer was a gaping wound that was already turning gray and black at the edges. It was now well into the category of being a chronic ulcer.
With the realm of possibilities large, they started with the man’s medical history. The man had immigrated to the US from Korea 20 years ago. He owned and worked at a laundromat, which involved standing for more than eight hours a day. He had a history of eczema on his legs, high cholesterol, high blood pressure, and Type 2 diabetes. For these, he was prescribed a statin for his cholesterol, two blood pressure medications (hydrochlorothiazide and losartan), and metformin for his diabetes. He told doctors he was not good at taking the regimen of medicine.
His diabetes was considered “poorly controlled.” A month prior, he had a glycated hemoglobin (A1C or HbA1C) test—which indicates a person’s average blood sugar level over the past two or three months. His result was 11 percent, while the normal range is between 4.2 and 5.6 percent.
His blood pressure, meanwhile, was 215/100 mm Hg at the emergency department. For reference, readings higher than 130/80 mm Hg on either number are considered the first stage of high blood pressure. Over the past three years, the man’s blood pressure had systolic readings (top number, pressure as heart beats) ranging from 160 to 230 mm Hg and diastolic readings (bottom number, pressure as heart relaxes) ranging from 95 to 120 mm Hg.
Clinical clues
Given the patient’s poorly controlled diabetes, a diabetic ulcer was initially suspected. But the patient didn’t have any typical signs of diabetic neuropathy that are linked to ulcers. These would include numbness, unusual sensations, or weakness. His responses on a sensory exam were all normal. Diabetic ulcers also typically form on the foot, not the lower leg.
X-rays of the ankle showed swelling in the soft tissue but without some signs of infection. The doctors wondered if the man had osteomyelitis, an infection in the bone, which can be a complication in people with diabetic ulcers. The large size and duration of the ulcer matched with a bone infection, as well as some elevated inflammatory markers he had on his blood tests.
To investigate the bone infection further, they admitted the man to the hospital and ordered magnetic resonance imaging (MRI). But the MRI showed only a soft-tissue defect and a normal bone, ruling out a bone infection. Another MRI was done with a contrast agent. That showed that the man’s large arteries were normal and there were no large blood clots deep in his veins—which is sometimes linked to prolonged standing, as the man did at his laundromat job.
As the doctors were still working to root out the cause, they had started him on a heavy-duty regimen of antibiotics. This was done with the assumption that on top of whatever caused the ulcer, there was now also a potentially aggressive secondary infection—one not knocked out by the previous round of antibiotics the man had been given.
With a bunch of diagnostic dead ends piling up, the doctors broadened their view of possibilities, newly considering cancers, rare inflammatory conditions, and less common conditions affecting small blood vessels (as the MRI has shown the larger vessels were normal). This led them to the possibility of a Martorell’s ulcer.
These ulcers, first described in 1945 by a Spanish doctor named Fernando Martorell, form when prolonged, uncontrolled high blood pressure causes the teeny arteries below the skin to stiffen and narrow, which blocks the blood supply, leading to tissue death and then ulcers. The ulcers in these cases tend to start as red blisters and evolve to frank ulcers. They are excruciatingly painful. And they tend to form on the lower legs, often over the Achilles’ tendon, though it’s unclear why this location is common.
What the doctor ordered
The doctors performed a punch biopsy of the man’s ulcer, but it was inconclusive—which is common with Martorell’s ulcers. The doctors turned to a “deep wedge biopsy” instead, which is exactly what it sounds like.
A pathology exam of the tissue slices from the wedge biopsy showed blood vessels that had thickened and narrowed. It also revealed extensive inflammation and necrosis. With the pathology results as well as the clinical presentation, the doctors diagnosed the man with a Martorell’s ulcer.
They also got back culture results from deep-tissue testing, finding that the man’s ulcer had also become infected with two common and opportunistic bacteria—Serratia marcescens and Enterococcus faecalis. Luckily, these are generally easy to treat, so the doctors scaled back his antibiotic regimen to target just those germs.
The man underwent three surgical procedures to clean out the dead tissue from the ulcer, then a skin graft to repair the damage. Ultimately, he made a full recovery. The doctors at first set him on an aggressive regimen to control his blood pressure, one that used four drugs instead of the two he was supposed to be taking. But the four-drug regimen caused his blood pressure to drop too low, and he was ultimately moved back to his original two-drug treatment.
The finding suggests that if he had just taken his original medications as prescribed, he would have kept his blood pressure in check and avoided the ulcer altogether.
In the end, “the good outcome in this patient with a Martorell’s ulcer underscores the importance of blood-pressure control in the management of this condition,” the doctors concluded.
Beth is Ars Technica’s Senior Health Reporter. Beth has a Ph.D. in microbiology from the University of North Carolina at Chapel Hill and attended the Science Communication program at the University of California, Santa Cruz. She specializes in covering infectious diseases, public health, and microbes.
About two months after receiving a donated kidney, a 61-year-old man ended up back in the hospital. He was tired, nauseous, and vomiting. He was also excessively thirsty and producing too much urine. Over the next 10 days, things only got worse. The oxygen levels in his blood began to fall. His lungs filled with fluid. He kept vomiting. He couldn’t eat. Doctors inserted a feeding tube. His oxygen levels and blood pressure kept falling. He was admitted to the intensive care unit and put on mechanical ventilation. Still, things kept getting worse.
At that point, he was transferred to the ICU of Massachusetts General Hospital, where he had received the transplant. He was in acute respiratory failure and shock.
In a case report in this week’s issue of the New England Journal of Medicine, doctors at Mass General explained how they determined what was wrong with the man. Their first steps were collecting more information about the man’s symptoms from his wife, reviewing his family medical history, and contacting the regional organ-procurement organization that provided the kidney.
Process of elimination
The man’s condition and laboratory tests suggested he had some sort of infection. But as a transplant recipient who was on a variety of immunosuppressive drugs, the list of infectious possibilities was “extensive.”
Dr. Camille Kotton, Clinical Director of the hospital’s Transplant and Immunocompromised Host Infectious Diseases division, laid out her thinking. She started with a process of elimination. As an immunosuppressed transplant patient, he was also on several medications to proactively prevent infections. These would rule out herpesviruses and cytomegalovirus. He was also on a combination of antibiotics that would rule out many bacterial infections, as well as the fungal infection Pneumocystis jirovecii that strikes the immunocompromised and the protozoan parasite Toxoplasma gondii.
One feature stood out: The man had developed elevated levels of eosinophils, white blood cells that can increase for various reasons—including parasitic infections. The man also had a reddish-purple rash over his abdomen. Coupled with the severity of his illness, Kotton suspected a widespread parasitic infection.
The man’s history was notable for contact with domestic cats and dogs—including a cat scratch in the time between having the transplant and falling critically ill. But common bacterial infections linked to cat scratches could be ruled out. And other parasitic infections that might come from domestic animals in the US, such as toxocariasis, don’t typically lead to such critical illnesses.
The exercise group, which had supervised exercise for the first six months of the three-year intervention, reported more exercise over the study. At the end, the exercise group was averaging over 20 MET hours per week, while the education group’s average was around 15 MET hours per week. The exercise group also scored better at cardiorespiratory fitness and physical functioning.
Still, with the health education, the control group also saw a boost to their exercise during the trial, with their average starting around 10 MET hours per week. These findings “raise the possibility of an even more powerful effect of exercise on cancer outcomes as compared with a completely sedentary control group,” the researchers note.
For now, it’s not entirely clear how exercise keeps cancers at bay, but it squares with numerous other observational studies that have linked exercise to better outcomes in cancer patients. Researchers have several hypotheses, including that exercise might cause “increased fluid shear stress, enhanced immune surveillance, reduced inflammation, improved insulin sensitivity, and altered microenvironment of major sites of metastases,” the authors note.
In the study, exercise seemed to keep local and distant colon cancer from recurring, as well as prevent new cancers, including breast, prostate, and colorectal cancers.
Outside experts hailed the study’s findings. “This indicates that exercise has a similarly strong effect as previously shown for chemotherapy, which is really quite impressive,” Marco Gerlinger, a gastrointestinal cancer expert at Queen Mary University of London, said in a statement. “One of the commonest questions from patients is what they can do to reduce the risk that their cancer comes back. Oncologists can now make a very clear evidence-based recommendation.”
“Having worked in bowel cancer research for 30 years, this is an exciting breakthrough in the step-wise improvement in cure rates,” David Sebag-Montefiore, a clinical oncologist at the University of Leeds, said. “The great appeal of a structured moderate intensity exercise is that it offers the benefits without the downside of the well-known side effects of our other treatments.”
When an 84-year-old man in Hong Kong was admitted to a hospital for a condition related to an enlarged prostate, doctors noticed something else about him—he was oddly gray, according to a case report in the New England Journal of Medicine.
His skin, particularly his face, had an ashen appearance. His fingernails and the whites of his eyes had become silvery. When doctors took a skin biopsy, they could see tiny, dark granules sitting in the fibers of his skin, in his blood vessels, in the membranes of his sweat glands, and in his hair follicles.
A blood test made clear what the problem was: the concentration of silver in his serum was 423 nmol/L, over 40 times the reference level for a normal result, which is less than 10 nmol/L. The man was diagnosed with a rare case of generalized argyria, a buildup of silver in the body’s tissue that causes a blueish-gray discoloration—which is generally permanent.
When someone consumes silver particles, the metal moves from the gut into the bloodstream in its ionic form. It’s then deposited throughout the body in various tissues, including the skin, muscles, heart, lungs, liver, spleen, and kidneys. There’s some evidence that it accumulates in at least parts of the brain as well.
Discoloration becomes apparent in tissues exposed to sunlight—hence the patient’s notably gray face. Silver ions in the skin undergo photoreduction from ultraviolet light exposure, forming atomic silver that can be oxidized to compounds such as silver sulfide and silver selenide, creating a bluish-gray tinge. Silver can also stimulate the production of the pigment melanin, causing darkening. Once discoloration develops, it’s considered irreversible. Chelation therapy—generally used to remove metals from the body—is ineffective against argyria. That said, some case studies have suggested that laser therapy may help.
If Margaritaville were a real place, it should definitely keep a few dermatologists on hand.
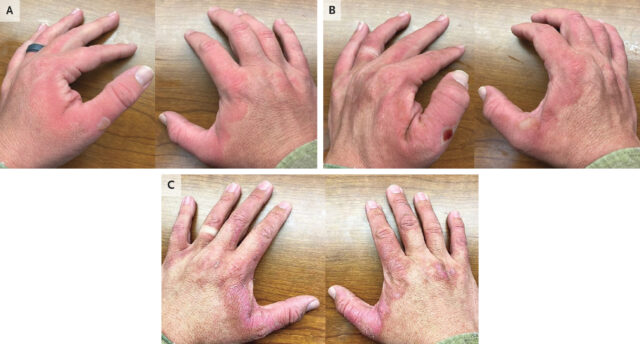
In a case of an oft-overlooked food preparation risk, a 40-year-old man showed up to an allergy clinic in Texas with a severe, burning rash on both his hands that had two days earlier. A couple of days later, it blistered. And a few weeks after that, the skin darkened and scaled. After several months, the skin on his hands finally returned to normal.
The culprit: lime juice and sunlight.
It turns out that just before developing the nasty skin eruption, the man had manually squeezed a dozen limes, then headed to an outdoor soccer game without applying sunscreen. His doctors diagnosed the man’s rash as a classic case of phytophotodermatitis, according to a case report published Wednesday in the New England Journal of Medicine.
The condition is caused by toxic substances found in plants (phyto) that react with UV light (photo) to cause a burning, blistering, scaling, pigmented skin condition (dermatitis).
Specifically, the toxic chemicals are furocoumarins, which are found in some weeds and also a range of plants used in food. Those include celery, carrot, parsley, fennel, parsnip, lime, bitter orange, lemon, grapefruit, and sweet orange. Furocoumarins include chemicals with linear structures, psoralens, and angular structures, called angelicins, though not all of them are toxic.
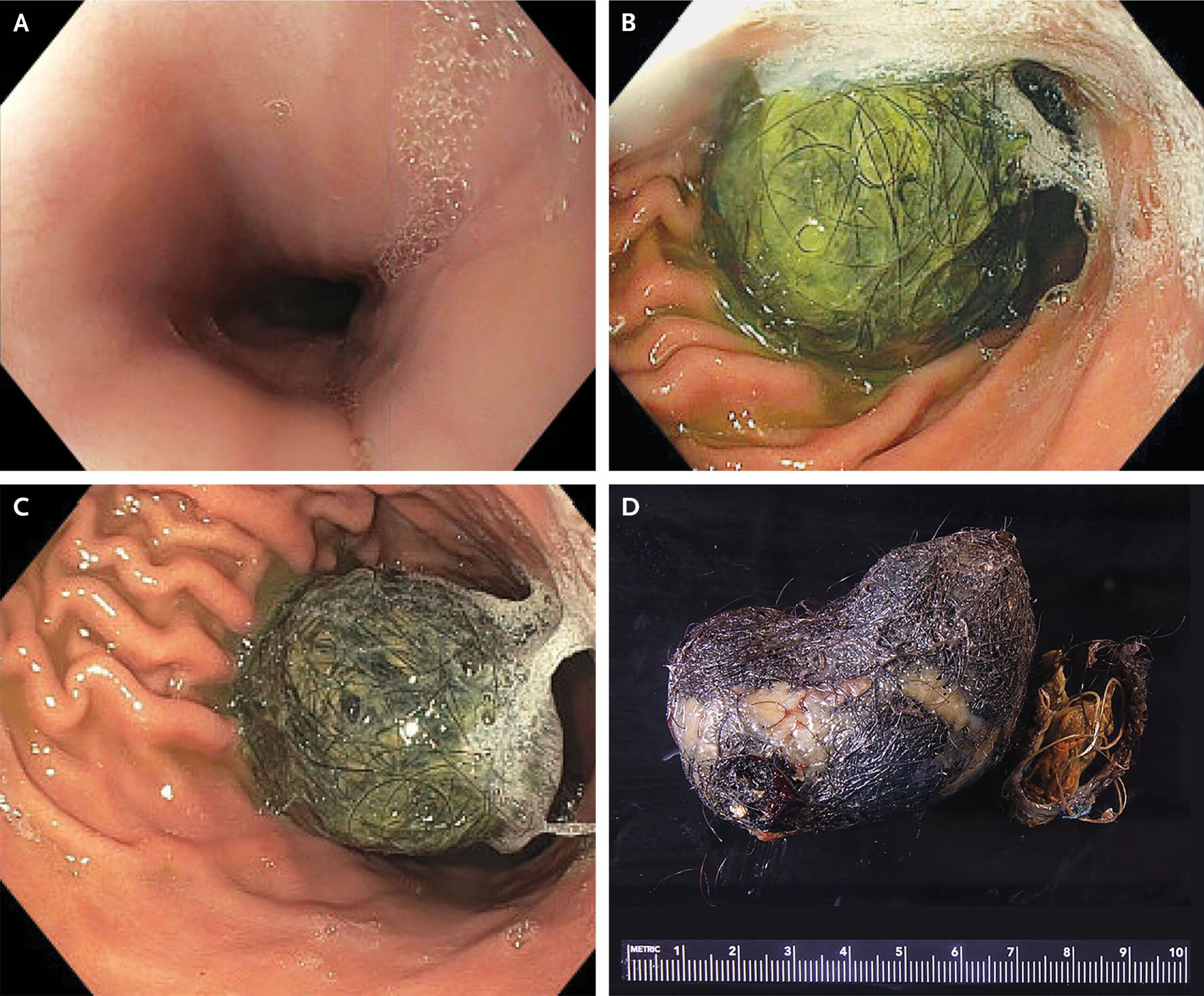
Hair is resistant to digestion and isn’t easily moved through the digestive system. As such, it often gets lodged in folds of the gastric lining, denatures, and then traps food and gunk to form a mass. Over time, it will continue to collect material, growing into a thick, matted wad.
Of all the bezoars, trichobezoars are the most common. But none of them are particularly easy to spot. On CT scans, bezoars can be indistinguishable from food in the stomach unless there’s an oral contrast material. To look for a possible bezoar in the teen, her doctors ordered an esophagogastroduodenoscopy, in which a scope is put down into the stomach through the mouth. With that, they got a clear shot of the problem: a trichobezoar. (The image is here, but a warning: it’s graphic).
Tangled tail
But this trichobezoar was particularly rare; hair from the mottled mat had dangled down from the stomach and into the small bowel, which is an extremely uncommon condition called Rapunzel syndrome, named after the fairy-tale character who lets down her long hair. It carries a host of complications beyond acute abdominal pain, including perforation of the stomach and intestines, and acute pancreatitis. The only resolution is surgical removal. In the teen’s case, the trichobezoar came out during surgery using a gastrostomy tube. Surgeons recovered a hairball about 2.5 inches wide, along with the dangling hair that reached into the small intestine.
For any patient with a trichobezoar, the most important next step is to address any psychiatric disorders that might underlie hair-eating behavior. Hair eating is often linked to a condition called trichotillomania, a repetitive behavior disorder marked by hair pulling. Sometimes, the disorder can be diagnosed by signs of hair loss—bald patches, irritated scalp areas, or hair at different growth stages. But, for the most part, it’s an extremely difficult condition to diagnose as patients have substantial shame and embarrassment about the condition and will often go to great lengths to hide it.
Another possibility is that the teen had pica, a disorder marked by persistent eating of nonfood, nonnutritive substances. Intriguingly, the teen noted that she had pica as a toddler. But doctors were skeptical that pica could explain her condition given that hair was the only nonfood material in the bezoar.
The teen’s doctors would have liked to get to the bottom of her condition and referred her to a psychiatrist after she successfully recovered from surgery. But unfortunately, she did not return for follow-up care and told her doctors she would instead see a hypnotherapist that her friends recommended.
The human body is full of marvels, some even bordering on miraculous. That includes the limited ability for nerves to regenerate after injuries, allowing people to regain some function and feeling. But that wonder can turn, well, unnerving when those regenerated wires end up in a jumble.
Such is the case for a rare neurological condition called gustatory hyperhidrosis, also known as Frey’s syndrome. In this disorder, nerves regenerate after damage to either of the large saliva glands that sit on either side of the face, just in front of the ears, called the parotid glands. But that nerve regrowth goes awry due to a quirk of anatomy that allows the nerves that control saliva production for eating to get tangled with those that control sweating for temperature control.
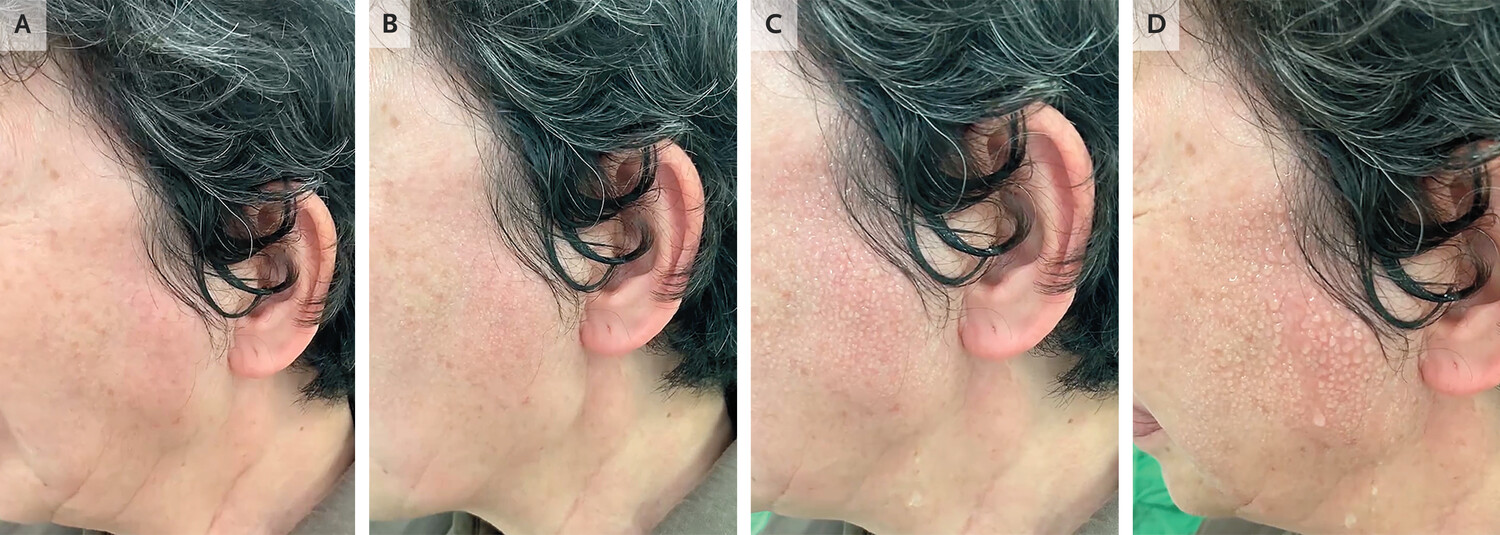
In this week’s issue of the New England Journal of Medicine, doctors in Taiwan report an unusual presentation of the disorder in a 76-year-old woman. She told doctors that, for two years, every time she ate, her face would begin profusely sweating. In the clinic, the doctors observed the phenomenon themselves. They watched as she took a bite of pork jerky and began chewing.
Enlarge/ Panel A, 10 seconds after beginning chewing; Panel B, 30 seconds after; Panel C, 50 seconds after; and Panel D, 75 seconds after.
At the start, her face was dry and had a normal tone. But, within 30 seconds, her left cheek began to glisten with sweat and turn red from flushing. By 50 seconds, large beads of sweat coated her cheek. At 75 seconds, droplets ran down her cheek and onto her neck.
Anatomy quirk
Seven years before that doctor’s appointment, the woman had undergone surgery to remove the parotid gland on that side of her face due to the growth of a benign tumor. Gustatory hyperhidrosis is a common complication after such a removal, called a parotidectomy. Some published studies estimate that up to 96 percent of parotidectomy patients will go on to develop the disorder. But, if it does develop, it usually does so within about six to 18 months after the surgery—the time it can take for nerves to regrow. But, in the woman’s case, it appeared to develop after five years since she reported that it started only two years prior to her appointment. It’s unclear why there was such a delay.
Doctors hypothesize that gustatory hyperhidrosis develops after salivary gland injuries or surgeries because of the way nerve fibers are bundled in that part of the head. The nerves that control the salivary glands are part of the parasympathetic nervous system (PSNS). This division of the nervous system is sometimes described as controlling the relatively calm “rest and digest” bodily functions, which are controlled unconsciously as part of the autonomic nervous system that controls things like heart rate.
The PSNS is in contrast to the other part of the autonomic nervous system, called the sympathetic nervous system (SNS). The SNS controls the unconscious “fight or flight” stress responses, which include sweat glands.
Tangled fibers
While PSNS fibers that control the saliva glands and SNS fibers that control sweat glands are from different divisions, they come together on the side of the face. Specifically, they meet up in a tributary nerve called the auriculotemporal nerve. And, they don’t just feed into the same physical conduit, they also overlap in their chemical regulation. Often SNS and PSNS fibers are activated by different signaling molecules (aka neurotransmitters). But it just so happens that the nerve fibers that control sweat glands are activated by the same neurotransmitter that activates the fibers in the PSNS, including those regulating saliva glands. They’re both regulated by a neurotransmitter called acetylcholine.
When PSNS and SNS nerve fibers are damaged near the parotid salivary gland from injury or surgery, the nerves can regenerate. But, given their physical and chemical overlaps, doctors think that in gustatory hyperhidrosis, PSNS nerve fibers end up growing back abnormally, along the paths of SNS fibers. This ends up connecting the PSNS fibers to sweat glands in the skin. So, upon signals of eating, the crossed nerve fibers lead not to salivation but heat responses, including sweat production and blood vessel dilation, which explains the facial flushing.
Living with it
Thankfully, there are various treatments for people with gustatory hyperhidrosis. They include surgical reconstruction or injections of Botox (botulinum neurotoxin), which can shut down the activity of the sweat glands. Similarly, there are topical anticholinergics, which block and inhibit the activity of acetylcholine, the neurotransmitter that activates the nerve fibers activating the sweat glands. There are also topical antiperspirants that can help.
After the doctors in Taiwan diagnosed their patient with gustatory hyperhidrosis, they discussed these options with her. But she reportedly “opted to live with the symptoms.”
In what may be the biological equivalent to getting struck by lightning, a very unlucky man in the Philadelphia area took a very rare bee sting directly to the eyeball—and things went badly from there.
As one might expect, the 55-year-old went to the emergency department, where doctors tried to extract the injurious insect’s stinger from the man’s right eye. But it soon became apparent that they didn’t get it all.
Two days after the bee attack, the man went to the Wills Eye Hospital with worsening vision and pain in the pierced eye. At that point, the vision in his right eye had deteriorated to only being able to count fingers. The eye was swollen, inflamed, and bloodshot. Blood was visibly pooling at the bottom of his iris. And right at the border between the man’s cornea and the white of his eye, ophthalmologists spotted the problem: a teeny spear-like fragment of the bee’s stinger still stuck in place.
(Images of the eye and stinger fragment are here for those who aren’t squeamish. The white arrow in Panel A shows the location of the stinger fragment while the asterisk marks the pooled blood.)
Get thee to an ophthalmologist
In a report published recently in the New England Journal of Medicine, treating ophthalmology experts Talia Shoshany and Zeba Syed made a critical recommendation: If you happen to be among the ill-fated few who are stung in the eye by a bee, you should make sure to see an eye doctor specifically.
“I am not surprised that the ER missed a small fragment,” Shoshany told Ars over email. “They pulled out the majority of the stinger, but the small fragment was only able to be visualized at a slit lamp,” she said, referring to a microscope with a bright light used in eye exams. In this case, they visualized the stinger at 10X or 16X magnification with the additional help of a fluorescent dye. Moreover, after spotting it, the stinger fragment “needed to be pulled out with ophthalmic-specific micro-forceps.”
After finally getting the entirety of the wee dagger out, Shoshany and Syed prescribed a topical antibacterial and prednisolone eye drops (a steroid for inflammation). At a five-month follow-up, the patient had recovered and the vision in his right eye had improved to 20/25.
For those now in fear of eye stings, Soshany has some comforting words: “Ocular bee stings are very rare.” She noted this was the first one she had seen in her career. Although there are documented cases in the scientific literature, the incidence rate is unknown. The odds of getting struck by lightning, meanwhile, are 1 in 15,300, according to the National Weather Service.
But one troubling aspect of this case is that it’s unclear why the man was stung to begin with. According to Shoshany, the man worked on a property with a beehive, but he didn’t work with the insects himself. “He reports he was just walking by and several bees flew up to him; one stung him in the eye,” she said. It’s unclear what provoked them.
Most of the time, when kids accidentally gulp down a non-edible object, it travels toward the stomach. In the best-case scenarios for these unfortunate events, it’s a small, benign object that safely sees itself out in a day or two. But in the worst-case scenarios, it can go down an entirely different path.
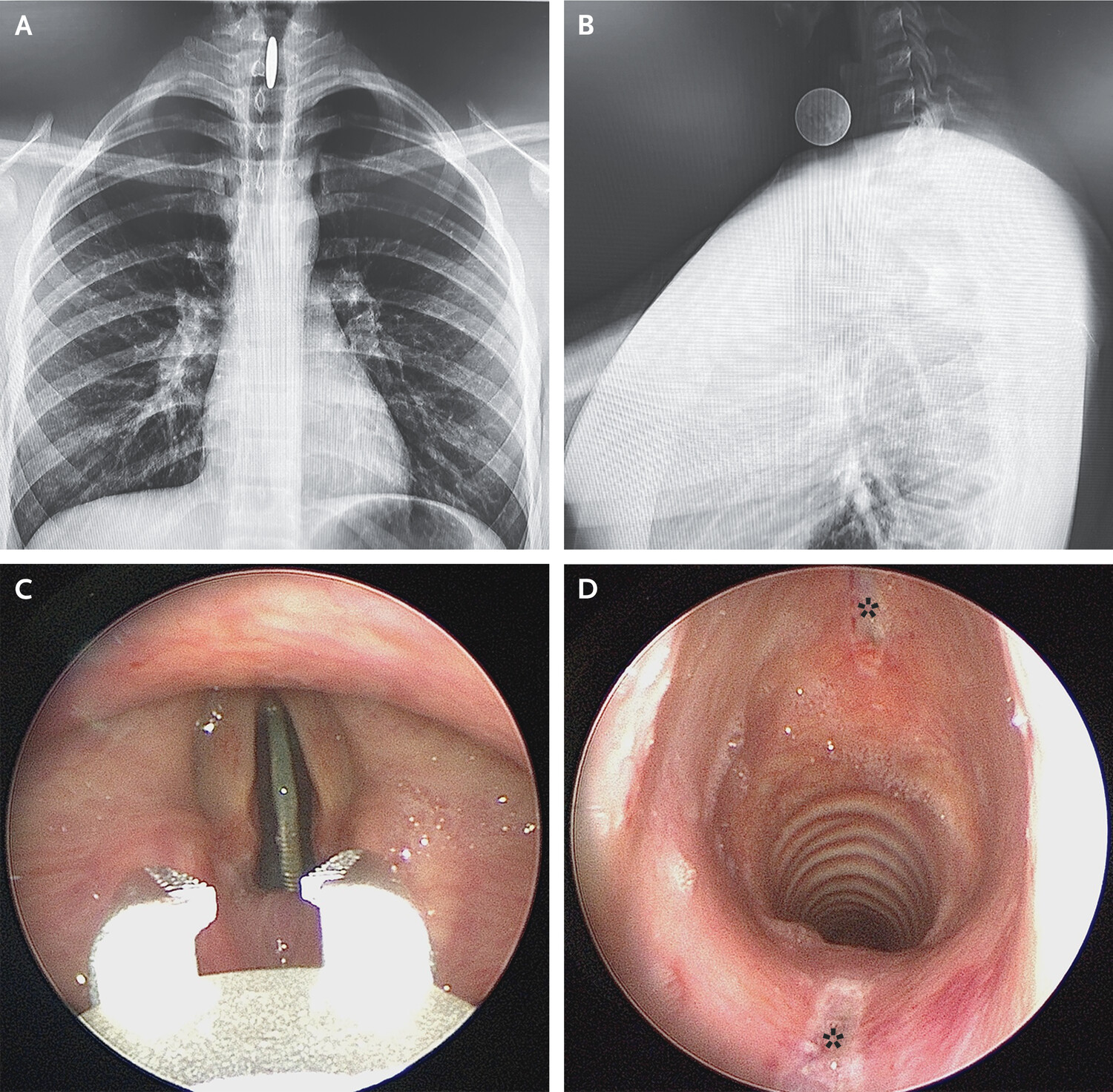
That was the case for a poor teen in California, who somehow swallowed a quarter. The quarter didn’t head down the esophagus and toward the stomach, but veered into the airway, sliding passed the vocal cords like they were a vending-machine coin slot.
Enlarge/ Radiographs of the chest (Panel A, postero- anterior view) and neck (Panel B, lateral view). Removal with optical forceps (Panel C and Video 1), and reinspection of ulceration (Panel D, asterisks)
In a clinical report published recently in the New England Journal of Medicine, doctors who treated the 14-year-old boy reported how they found—and later retrieved—the quarter from its unusual and dangerous resting place. Once it passed the vocal cords and the glottis, the coin got lodged in the subglottis, a small region between the vocal cords and the trachea.
Luckily, when the boy arrived at the emergency department, his main symptoms were hoarseness and difficulty swallowing. He was surprisingly breathing comfortably and without drooling, they noted. But imaging quickly revealed the danger his airway was in when the vertical coin lit up his scans.
“Airway foreign bodies—especially those in the trachea and larynx—necessitate immediate removal to reduce the risk of respiratory compromise,” they wrote in the NEJM report.
The teen was given general anesthetic while doctors used long, optical forceps, guided by a camera, to pluck the coin from its snug spot. After grabbing the coin, they re-inspected the boy’s airway noting ulcerations on each side matching the coin’s ribbed edge.
After the coin’s retrieval, the boy’s symptoms improved and he was discharged home, the doctors reported.
It’s hard to imagine a more common stressor for new parents than the recurring riddle: Why is the baby crying? Did she just rub her eyes—tired? Is he licking his lips—hungry? The list of possible culprits and vague signs, made hazier by brutal sleep deprivation, can sometimes feel endless. But for one family in New England, the list seemed to be swiftly coming to an end as their baby continued to slip away from them.
According to a detailed case report published today in the New England Journal of Medicine, it all started when the parents of an otherwise healthy 8-week-old boy noticed that he started crying more and was more irritable. This was about a week before he would end up in the pediatric intensive care unit (PICU) of the Massachusetts General Hospital.
His grandmother, who primarily cared for him, noticed that he seemed to cry more vigorously when the right side of his abdomen was touched. The family took him to his pediatrician, who could find nothing wrong upon examination. Perhaps it was just gas, the pediatrician concluded—a common conclusion.
Rapid decline
But when the baby got home from the doctor’s office, he had another crying session that lasted hours, which only stopped when he fell asleep. When he woke, he cried for eight hours straight. He became weaker; he had trouble nursing. That night, he was inconsolable. He had frantic arm and leg movements and could not sleep. He could no longer nurse, and his mother expressed milk directly into his mouth. They called the pediatrician back, who directed them to take him to the emergency room
There, he continued to cry, weakly and inconsolably. Doctors ordered a series of tests—and most were normal. His blood tests looked good. He tested negative for common respiratory infections. His urinalysis looked fine, and he passed his kidney function test. X-rays of his chest and abdomen looked normal, ultrasound of his abdomen also found nothing. Doctors noted he had high blood pressure, a fast heart rate, and that he hadn’t pooped in two days. Throughout all of the testing, he didn’t “attain a calm awake state,” the doctors noted. They admitted him to the hospital.
Four hours after he first arrived at the emergency department, he began to show signs of lethargy. Meanwhile, magnetic resonance imaging of his head found nothing. A lumbar puncture showed possible signs of meningitis—high red-cell count and protein levels—and doctors began courses of antibiotics in case that was the cause.
Six hours after his arrival, he began losing the ability to breathe. His oxygen saturation had fallen from an initial 97 percent to an alarming 85 percent. He was put on oxygen and transferred to the PICU. There, doctors noted he was difficult to arise, his head bobbed, his eyelids drooped, and he struggled to take in air. His cry was weak, and he made gurgling and grunting noises. He barely moved his limbs and couldn’t lift them against gravity. His muscles went floppy. Doctors decided to intubate him and start mechanical ventilation.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}