ADHD med shortages push DEA to up drug allotment by 23.5%
drug boost —
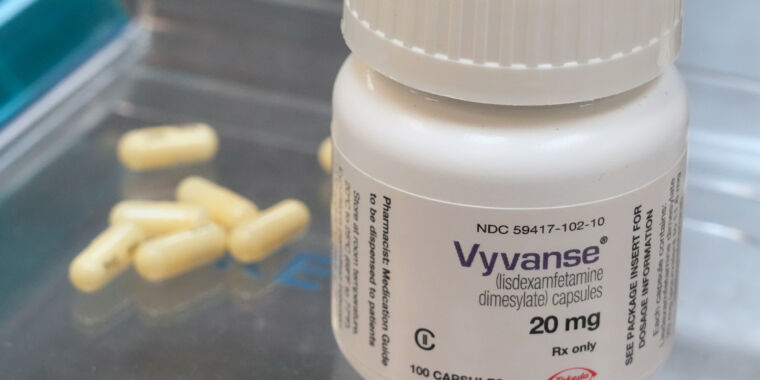
The DEA’s quota increase is for Vyvanse and its generic forms.
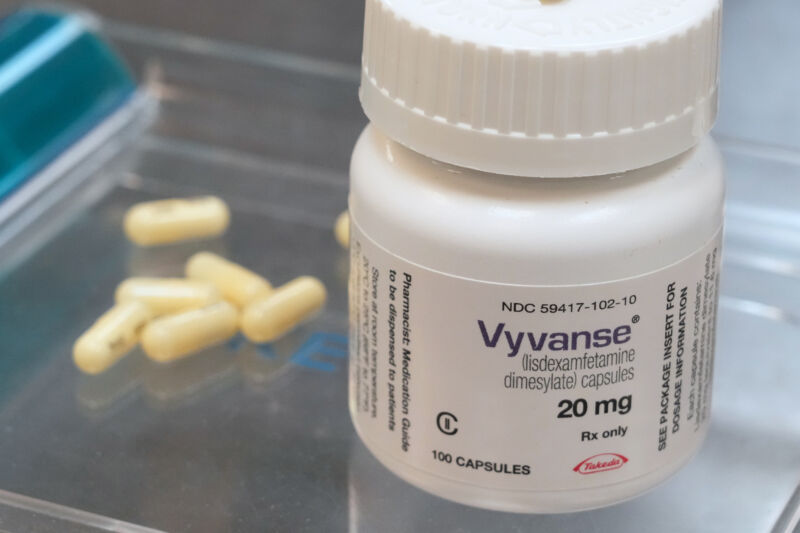
While supplies of Adderall and its generic versions are finally recovering after a yearslong shortage, the Drug Enforcement Administration is now working to curb the short supply of another drug for attention-deficit/hyperactivity disorder: Vyvanse (lisdexamfetamine) and its generic versions.
This week, the DEA said it will increase the allowed production amount of lisdexamfetamine by roughly 23.5 percent, increasing the current 26,500 kg quota by 6,236 kg, for a new total of 32,736 kg. The DEA also allowed for a corresponding increase in d-amphetamine, which is needed for production of lisdexamfetamine.
“These adjustments are necessary to ensure that the United States has an adequate and uninterrupted supply of lisdexamfetamine to meet legitimate patient needs both domestically and globally,” the DEA said.
Quotas
Just like Adderall (amphetamine/dextroamphetamine salts), Vyvanse (lisdexamfetamine) is an amphetamine-class stimulant classified by the DEA as a Schedule II drug. As such, the DEA controls its production levels to ensure demand is met while preventing excess supply that could find its way to the black market. The administration does this by setting an “aggregate production quota”—which is what the DEA adjusted for lisdexamfetamine this week—and doling out undisclosed allotments to drug manufacturers.
While various factors have contributed to the shortages of ADHD medications, some medical and industry groups have placed blame on the DEA’s quota system for underestimating demand and choking supply. For instance, the Adderall shortage began in 2022 following a labor shortage on the product’s production line at Teva, Adderall’s maker. But, while that production snag was resolved, prescription rates increased significantly, in part due to increased awareness of ADHD, broadening diagnosis criteria, and an increase in access with the rise of telehealth services, which boomed during the COVID-19 pandemic. In a report earlier this year, the American Society of Health-System Pharmacists pointed to the DEA’s quotas, saying they’re “exacerbating” shortages.
In an August 2023 joint letter, the DEA and the FDA responded to such criticism, suggesting that the quotas aren’t to blame. Rather, it’s that some manufacturers are not using up their allotment of controlled drugs.
“Based on DEA’s internal analysis of inventory, manufacturing, and sales data submitted by manufacturers of amphetamine products [which include the two ADHD drugs], manufacturers only sold approximately 70 percent of their allotted quota for the year, and there were approximately 1 billion more doses that they could have produced but did not make or ship. Data for 2023 so far show a similar trend,” the FDA and DEA wrote.
The FDA and DEA said they would work with manufacturers to ensure they would ramp up production of drugs in short supply or relinquish their remaining allotments.
Vyvanse shortage
A similarly complicated situation is seen with the current shortfall of Vyvanse and its generics. The DEA raised the quota after prodding from the Food and Drug Administration. In July, the FDA sent the DEA a letter requesting a quota increase. However, the shortage had actually begun in June 2023. At that time, Vyvanse’s maker, Takeda, said that a “manufacturing delay compounded by increased demand” had led to low inventory.
In August 2023, the FDA approved multiple generic versions of Vyvanse after Takeda’s patent exclusivity expired, raising hopes that the shortage would ease with the injection of new generics. But supply problems have persisted. In November, the Association for Accessible Medicines, which represents generic drugmakers, sent a letter to the DEA saying that generic manufacturers weren’t able to obtain enough raw material to “launch their products at full commercial scale,” because the quotas were standing in the way, according to reporting by Bloomberg.
FiercePharma reported another potential factor raised by lawmakers and industry watchers. Those onlookers took note of the timing of Takeda’s “manufacturing delays” just months before generics entered the market. With the significantly thinner profit margin of generic and off-patent drugs, there’s concern that manufacturers may de-prioritize production.
Last, the DEA flagged yet another factor in the supply chain: exports to foreign markets. While the FDA estimated a 6 percent increase in the domestic need for lisdexamfetamine between 2023 and 2024, the DEA’s export data showed a 34 percent increase in exports of lisdexamfetamine between 2022 and 2023, with expectations that exports would continue to increase this year and beyond. As such, the current 23.5 percent quota increase for lisdexamfetamine is only partly for domestic production. In fact, only a quarter of the 6,236 kg is intended for the US. Of the increased allotment, 1,558 kg is for domestic drug production, while the other 4,678 kg addresses increases in foreign demand, the DEA said.
ADHD med shortages push DEA to up drug allotment by 23.5% Read More »



{kind=link}
{kind=link}