The National Cancer Institute is using federal funds to study whether cancer can be cured by ivermectin, a cheap, off-patent anti-parasitic and deworming drug that fringe medical groups falsely claimed could treat COVID-19 during the pandemic and have since touted as a cure-all.
Large, high-quality clinical trials have resoundingly concluded that ivermectin is not effective against COVID-19. And there is no old or new scientific evidence to support a hypothesis that ivermectin can cure cancer—or justify any such federal expenditure. But, under anti-vaccine Health Secretary Robert F. Kennedy Jr.—who is otherwise well-known for claiming to have a parasitic worm in his brain—numerous members of the medical fringe are now in powerful federal positions or otherwise hold sway with the administration.
During a January 30 event, Anthony Letai, a cancer researcher the Trump administration installed as the director of the NCI in September, said the NCI was pursuing ivermectin.
“There are enough reports of it, enough interest in it, that we actually did—ivermectin, in particular—did engage in sort of a better preclinical study of its properties and its ability to kill cancer cells and we’ll probably have those results in a few months. So we are taking it seriously.”
The comments were highlighted today in a report from KFF Health News. Ars Technica was also at the event, “Reclaiming Science: The People’s NIH,” which was hosted by the MAHA [Make America Healthy Again] Institute. In the rest of his comments, Letai seemed to make a noticeable effort to temper expectations while also trying to avoid offending any ivermectin believers. “It’s not going to be a cure-all for cancer,” he said. At another point, he said that even if there are signals of anti-cancer properties in the preclinical studies, “I can tell you again, it’s not a really strong signal.”
Having a health insurance plan with a high deductible could not only cost you—it could also kill you.
A new study in JAMA Network Open found that people who faced those high out-of-pocket costs as well as a cancer diagnosis had worse overall survival and cancer-specific survival than those with more standard health plans.
The findings, while perhaps not surprising, are a stark reminder of the fraught decisions Americans face as the price of health care only continues to rise, and more people try to offset costs by accepting insurance plans with higher deductibles—that is, higher out-of-pocket costs they have to pay before their health insurance provider starts paying its share.
The issue is particularly critical right now for people who have insurance plans through the Affordable Care Act marketplace. Prices for those plans have skyrocketed this year after Congress failed to extend critical tax credits. Without those credits, monthly premiums for ACA plans have, on average, more than doubled. Early data on ACA enrollments for 2026 not only suggests that fewer people are signing up for the plans, but also that those who are enrolling are often choosing bronze plans, which are high-deductible plans.
In the study, researchers considered plans to be “high-deductible health plans” (HDHPs) if their deductibles were at least $1,200 to $1,350 for individuals or $2,400 to $2,700 for families between 2011 and 2018 (with the cutoffs increasing within the ranges during that time). For context, the average individual deductible for an ACA bronze plan in 2026 is about $7,500, according to KFF.
Risky plans
Based on previous data, such high out-of-pocket costs are known to lead people to delay or decrease health care—they may skip doctor visits, put off diagnostics, and avoid treatments. But for the new study, researchers led by Justin Barnes at Mayo Clinic in Rochester, Minnesota, wanted to know, more directly, if the plans were linked to lower survival— specifically for cancer patients, who obviously need more care than others.
Previous data from the trial reported that 107 participants received the mRNA vaccine and Keytruda treatment, while the remaining 50 only received Keytruda. At the two-year follow-up, 24 of the 107 (22 percent) who got the experimental vaccine and Keytruda had recurrence or death, while 20 of 50 (40 percent) treated with just Keytruda had recurrence or death, indicating a 44 percent risk reduction. The companies did not report the breakdown of the two groups in the press release this week for the five-year follow-up, but said the risk reduction was 49 percent, which is also what the companies reported for the three-year follow-up.
As for side effects, the companies reported that little had changed from previous analyses; adverse events were similar between the two groups. The top side effects linked to the vaccine were fatigue, injection site pain, and chills.
The results “highlight the potential of a prolonged benefit” of the vaccine combined with Keytruda in patients with high-risk melanoma,” Kyle Holen, a senior vice president at Moderna, said.
They also “illustrate mRNA’s potential in cancer care,” he said, noting that the company has eight more Phase 2 and Phase 3 trials going for mRNA vaccines against a variety of other cancers, including lung, bladder, and kidney cancers.
Marjorie Green, a senior vice president at Merck, called the five-year follow-up data a “meaningful milestone” and “encouraging.”
“[W]e look forward to late-stage data from the INTerpath clinical development program with Moderna, across a range of tumor types where significant unmet needs remain,” she said.
While the top-line results appear positive, conclusions can’t be drawn until the full data from the trial are published. The vaccines are also being developed amid a political environment hostile to mRNA vaccines. Anti-vaccine Health Secretary Robert F. Kennedy Jr. has railed against mRNA COVID-19 vaccines, making false claims about their safety and efficacy. In August, Kennedy unilaterally canceled $500 million in grant funding for the development of mRNA-based vaccines against diseases that pose pandemic threats.
The director of a federal health institute that has arguably produced two of the most controversial government studies in recent years has accepted a new federal role to advance the goals of the Make America Healthy Again movement. Meanwhile, the person replacing him as director is a close friend of Vice President JD Vance and was installed in a process that experts describe as completely outside standard hiring practices.
The series of events—revealed in an email to staff last week from the National Institutes of Health Director Jay Bhattacharya—is only exacerbating the spiraling fears that science is being deeply corrupted by politics under the Trump administration.
Richard Woychik, a molecular geneticist, is the outgoing director of the NIH’s National Institute of Environmental Health Sciences (NIEHS), which is located in Research Triangle Park, North Carolina. He has been director since 2020 and was recently appointed to a second five-year term, according to Science magazine. Woychik was hired at the institute in 2010, when he joined as deputy director, and was appointed acting director in 2019.
As the director of NIEHS, Woychik was also the director of the National Toxicology Program (NTP). This is an interagency program that has produced two highly controversial scientific reports during Woychik’s time in NIEHS’s upper leadership. One, initially released in 2016, claimed that cellphone radiation causes cancer based on findings from rats, though only male rats. The final reports were published in 2018. Another controversial study, finalized this year, suggested that high levels of fluoride lower the IQ of children. Both the cellphone radiation and fluoride studies have been roundly criticized for flaws in their methodology and analysis, and the scientific community has largely dismissed them.
However, the studies align with—and bolster—the conspiracy theories and misinformation spread by the MAHA movement, which is led by ardent anti-vaccine activist and current US health secretary Robert F. Kennedy Jr. As health secretary, Kennedy has pledged to remove fluoride from municipal water, which, over decades, has proven safe and highly effective at preventing tooth decay in children. He has also, at various times, suggested 5G cell phone radiation causes cancer, a variety of other health conditions, changes to DNA, and is used as mass surveillance.
Despite touting ambitious goals of making America healthier, the Trump administration on Monday revealed in court documents that it is backpedaling on a ban on cancer-causing asbestos.
Last year, under the Biden administration, the Environmental Protection Agency took a long-awaited step to ban the last type of asbestos still used in the US—chrysotile asbestos, aka “white asbestos.” While use of chrysotile asbestos was on the decline, the dangerous mineral has lingered in various gaskets, brake blocks, aftermarket automotive brakes and linings, other vehicle friction products, and some diaphragms used to make sodium hydroxide and chlorine.
With the ban, the US joined over 50 other countries around the world that had already banned its use due to health risks. Generally, asbestos is known to cause lung cancer, mesothelioma, ovarian cancer, and laryngeal cancer. Asbestos exposure is linked to more than 40,000 deaths in the US alone each year, the EPA noted at the time.
“The science is clear—asbestos is a known carcinogen that has severe impacts on public health. President Biden understands that this [is a] concern that has spanned generations and impacted the lives of countless people. That’s why EPA is so proud to finalize this long-needed ban on ongoing uses of asbestos,” Michael Regan, EPA administrator at the time, said in a statement.
“100% safe”
While the move was decades in the making and hailed by health proponents, it still allowed companies a generous period to phase out use of asbestos—in some cases up to 12 years. That didn’t stop industry from taking legal action against the regulation shortly after the EPA’s announcement. The litigation, brought by a number of companies and trade groups, including the American Chemistry Council, has been ongoing since then.
Doctors told the Times that they have already seen some cases where patients with treatable, early-stage cancers have delayed effective treatments to try ivermectin, only to see no effect and return to their doctor’s office with cancers that have advanced.
Risky business
Nevertheless, the malignant misinformation on social media has made its way into state legislatures. According to an investigation by NBC News published Monday, 16 states have proposed or passed legislation that would make ivermectin available over the counter. The intention is to make it much easier for people to get ivermectin and use it for any ailment they believe it can cure.
Idaho, Arkansas, and Tennessee have passed laws to make ivermectin available over the counter. On Monday, Louisiana’s state legislature passed a bill to do the same, and it now awaits signing by the governor. The other states that have considered or are considering such bills include: Alabama, Georgia, Kentucky, Maine, Minnesota, Mississippi, New Hampshire, North Carolina, North Dakota, Pennsylvania, South Carolina, and West Virginia.
State laws don’t mean the dewormer would be readily available, however; ivermectin is still regulated by the Food and Drug Administration, and it has not been approved for over-the-counter use yet. NBC News called 15 independent pharmacies in the three states that have laws on the books allowing ivermectin to be sold over the counter (Idaho, Arkansas, and Tennessee) and couldn’t find a single pharmacist who would sell it without a prescription. Pharmacists pointed to the federal regulations.
Likewise, CVS Health said its pharmacies are not currently selling ivermectin over the counter in any state. Walgreens declined to comment.
Some states, such as Alabama, have considered legislation that would protect pharmacists from any possible disciplinary action for dispensing ivermectin without a prescription. However, one pharmacist in Idaho, who spoke with NBC News, said that such protection would still not be enough. As a prescription-only drug, ivermectin is not packaged for retail sale. If it were, it would include over-the-counter directions and safety statements written specifically for consumers.
“If you dispense something that doesn’t have directions or safety precautions on it, who’s ultimately liable if that causes harm?” the pharmacist said. “I don’t know that I would want to assume that risk.”
It’s a risk people on social media don’t seem to be concerned with.
The answer lies in how quickly body size evolves. We found that birds and mammals that reached large sizes more rapidly have reduced cancer prevalence. For example, the common dolphin, Delphinus delphis evolved to reach its large body size—along with most other whales and dolphins (referred to as cetaceans) about three times faster than other mammals. However, cetaceans tend to have less cancer than expected.
Larger species face higher cancer risks but those that reached that size rapidly evolved mechanisms for mitigating it, such as lower mutation rates or enhanced DNA repair mechanisms. So rather than contradicting Cope’s rule, our findings refine it.
Larger bodies often evolve, but not as quickly in groups where the burden of cancer is higher. This means that the threat of cancer may have shaped the pace of evolution.
Humans evolved to our current body size relatively rapidly. Based on this, we would expect humans and bats to have similar cancer prevalence, because we evolved at a much, much faster rate. However, it is important to note that our results can’t explain the actual prevalence of cancer in humans. Nor is that an easy statistic to estimate.
Human cancer is a complicated story to unravel, with a plethora of types and many factors affecting its prevalence. For example, many humans not only have access to modern medicine but also varied lifestyles that affect cancer risk. For this reason, we did not include humans in our analysis.
Fighting cancer
Understanding how species naturally evolve cancer defences has important implications for human medicine. The naked mole rat, for example, is studied for its exceptionally low cancer prevalence in the hopes of uncovering new ways to prevent or treat cancer in humans. Only a few cancer cases have ever been observed in captive mole rats, so the exact mechanisms of their cancer resistance remain mostly a mystery.
At the same time, our findings raise new questions. Although birds and mammals that evolved quickly seem to have stronger anti-cancer mechanisms, amphibians and reptiles didn’t show the same pattern. Larger species had higher cancer prevalence regardless of how quickly they evolved. This could be due to differences in their regenerative abilities. Some amphibians, like salamanders, can regenerate entire limbs—a process that involves lots of cell division, which cancer could exploit.
Putting cancer into an evolutionary context allowed us to reveal that its prevalence does increase with body size. Studying this evolutionary arms race may unlock new insights into how nature fights cancer—and how we might do the same.
Two big, somewhat conflicting studies on alcohol risks will influence new guidelines.
Heavy drinking is clearly bad for your health. But it’s long been questioned whether moderate drinking is also risky—and, if so, how risky, exactly.
Health researchers have consistently found links between alcohol consumption and several types of cancers (namely mouth, throat, colon, rectal, liver, and breast), as well as liver diseases, injuries, and traffic accidents. But nailing down the health risks from the lower levels of drinking has been tricky. For one, much of the data on moderate drinking is from observational studies in different countries, cultures, and populations. They cannot determine if alcohol is the direct cause of any given association, and they may be swayed by other lifestyle factors. The resulting data can be noisy and inconsistent.
Moreover, many studies rely on people to self-report whether they drink and, if so, how much, which is problematic because people may not accurately assess and/or report how much they actually drink. A related problem is that studies in the past often compared drinkers to people who said they didn’t drink. But, the trouble is, non-drinking groups are often some mix of people who are lifelong abstainers and people who used to drink but quit for some reason—maybe because of health effects. This latter group has the potential to have lingering health effects from their drinking days, which could skew any comparisons looking for health differences.
Then there’s the larger, common problem with any research focused on food or beverages: some have been sponsored or somehow swayed by industry, casting suspicion on the findings, particularly the ones indicating benefits. This has been a clear problem for alcohol research. For instance, in 2018, the National Institutes of Health shut down a $100 million trial aimed at assessing the health effects (and potential benefits) of moderate drinking after it came to light that much of the funding was solicited from the alcohol industry. There was a lot of questionable communication between NIH scientists and alcohol industry representatives.
With all of that in the background, there’s been clamorous debate about how much risk, if any, people are swallowing with their evening cocktail, gameday beer, or wine with dinner.
Currently, the US dietary guidance recommends that if adults drink, they should stick to drinking in moderation, defined as “alcohol intake to two drinks or fewer in a day for men and one drink or fewer in a day for women.” But recently, health experts in the US and abroad have started calling for lower limits, noting that more data has poured in that fortifies links to cancers and other risks. In 2023, for instance, Canada released recommendations that people limit their alcohol consumption to two drinks or fewer per week—that’s down significantly from the previously recommended limit of 10 drinks per week for women and 15 drinks per week for men.
Two reviews
Now, it’s America’s turn to decide if they’ll set the bar lower, too. This year, the US will update its dietary guidelines, which are carried out by the Department of Health and Human Services and the Department of Agriculture every five years. The federal government has requested two big scientific reviews to assess the current knowledge of the health effects of alcohol, which will both inform any potential revisions to the alcohol guidelines. Now, both studies have been released and are open for discussion.
One is from the National Academies of Sciences, Engineering, and Medicine (the National Academies), which was tasked by Congress to review the current evidence on alcohol with a focus on how moderate drinking potentially affects a specific set of health outcomes. The review compared health outcomes in moderate drinkers with those of lifelong abstainers. For the review, the National Academies set up a committee of 14 experts.
Based on top-line takeaways and tone, the two reports seem to have very different findings. While the National Academies review found a mix of benefits and harms from moderate drinking (one drink per day for women, and two per day for men), the ICCPUD review suggested that even the smallest amounts of alcohol (one drink per week) increased risk of death and various diseases. However, a closer look at the data shows they have some common ground.
The National Academies review
First, for the National Academies’ review, experts found sufficient evidence to assess the effects of moderate drinking on all-cause mortality, certain cancers, and cardiovascular risks. On the other hand, the reviewers found insufficient evidence to assess moderate drinking’s impact on weight changes, neurocognition, and lactation-related risks.
For all-cause mortality, a meta-analysis of data from eight studies found that moderate drinkers had a 16 percent lower risk of all-cause mortality (death from any cause) compared with lifelong abstainers. A meta-analysis of three studies suggested the risk of all-cause mortality was 23 percent lower for females who drank moderately compared to never-drinking females. Data from four studies indicated that moderate drinking males had a 16 percent lower risk of all-cause mortality than never-drinking males. Additional analyses found that the risk of all-cause mortality was 20 percent lower for moderate drinkers less than age 60 and 18 percent lower for moderate drinkers age 60 and up.
“Based on data from the eight eligible studies from 2019 to 2023, the committee concludes that compared with never consuming alcohol, moderate alcohol consumption is associated with lower all-cause mortality,” the review states. The reviewers rated the conclusion as having “moderate certainty.”
Cancer and cardiovascular disease
For a look at cancer risks, a meta-analysis of four studies on breast cancer found that moderate drinkers had an overall 10 percent higher risk than non-drinkers. An additional analysis of seven studies found that for every 10 to 14 grams of alcohol (0.7 to one standard drink) consumed per day, there was a 5 percent higher risk of breast cancer. The data indicated that people who drank higher amounts of alcohol within the moderate range had higher risks than those who drank lower amounts in the moderate range (for instance, one drink a day versus 0.5 drinks a day).
For context, the average lifetime risk of being diagnosed with breast cancer in non-drinking females is about 11 to 12 percent. A 10 percent relative increase in risk would raise a person’s absolute risk to around 12 to 13 percent. The average lifetime risk of any female dying of breast cancer is 2.5 percent.
Overall, the reviewers concluded that “consuming a moderate amount of alcohol was associated with a higher risk of breast cancer,” and the conclusion was rated as having moderate certainty.
A meta-analysis on colorectal cancer risks found a “statistically nonsignificant higher risk” in moderate drinkers compared to non-drinkers. However, studies looking at alcohol consumption at the highest levels of moderate drinking for males (e.g., two drinks per day) suggested a higher risk compared to males who drank lower amounts of alcohol in the moderate range (one drink per day).
The review concluded that there was insufficient evidence to support a link between moderate drinking and oral cavity, pharyngeal, esophageal, and laryngeal cancers.
Finally, for cardiovascular risks, meta-analyses found moderate drinking was associated with a 22 percent lower risk of heart attacks and an 11 percent lower risk of stroke (driven by lower risk of ischemic stroke, specifically). The reviewers rated these associations as low certainty, though, after noting that there was some concern for risk of bias in the studies.
For cardiovascular disease mortality, meta-analyses of four studies found an 18 percent lower risk of death among moderate drinkers compared with non-drinkers. Broken down, there was a 23 percent lower risk in female drinkers and 18 percent lower risk in male drinkers. The lower risk of cardiovascular disease mortality was rated as moderate certainty.
The ICCPUD review
The ICCPUD subcommittee’s report offered a darker outlook on moderate drinking, concluding that “alcohol use is associated with increased mortality for seven types of cancer (colorectal, female breast, liver, oral cavity, pharynx, larynx, esophagus [squamous cell type]),” and “increased risk for these cancers begins with any alcohol use and increases with higher levels of use.”
The review modeled lifetime risks of cancer and death and relative risks for a long list of problems, including infectious diseases, non-communicable diseases, and injuries. Also, it didn’t just focus on non-drinkers versus moderate drinkers, but it assessed the relative risk of six levels of drinking: one drink a week; two drinks a week; three drinks a week; seven drinks a week (one a day); 14 drinks a week (two a day), and 21 drinks a week (three a day).
Overall, the analysis is very much a rough draft. There are some places where information is missing, and some of the figures are mislabeled and difficult to read. There are two figures labeled Figure 6, for instance and Figure 7 (which may be Figure 8), is a graph that doesn’t have a Y-axis, making it difficult to interpret. The study also doesn’t discuss the level of potential bias of individual studies in its analyses. It also doesn’t make note of statistically insignificant results, nor comment on the certainty of any of its findings.
For instance, the top-line summary states: “In the United States, males and females have a 1 in 1,000 risk of dying from alcohol use if they consume more than 7 drinks per week. This risk increases to 1 in 100 if they consume more than 9 drinks per week.” But a look at the modeling behind these estimates indicates the cutoffs of when drinkers would reach a 0.1 percent or 1 percent risk of dying from alcohol use are broad. For males, a 0.1 percent lifetime risk of an alcohol-attributed death is reached at 6.5 standard drinks, with a 95 percent confidence interval spanning less than one drink per week and 13.5 drinks per week. “This lifetime risk rose to 1 in 100 people above 8.5 drinks per week,” the text reads, but the confidence interval is again between one and 14 drinks per week. So, basically, at anywhere between about one and 14 drinks a week, a male’s lifetime risk of dying from alcohol may be either 0.1 or 1 percent, according to this modeling.
Death risks
Regarding risk of death, the study did not look at all-cause mortality, like the National Academies review. Instead, it focused on deaths from causes specifically linked to alcohol. For both males and females, modeling indicated that the total lifetime risk of any alcohol-attributed death for people who consumed one, two, three, or seven drinks per week was statistically non-significant (the confidence intervals for each calculation spanned zero). Among those who have 14 drinks per week, the total lifetime risk of death was about 4 in 100 from all causes, with unintentional injuries being the biggest contributor for males and liver diseases being the biggest contributor for females. Among those who have 21 drinks per week, the risk of death was about 7 in 100 for males and 8 in 100 for females. Unintentional injuries and liver diseases were again the biggest contributors to the risk.
Some experts have speculated that the lower risk of all-cause mortality found in the National Academies’ analysis (which has been seen in previous studies) may be due to healthy lifestyle patterns among people who drink moderately rather than the protective effects of alcohol. The line of thinking would suggest that healthy lifestyle choices, like regular exercise and a healthy diet, can negate certain risks, including the potential risks of alcohol. However, the ICCPUD emphasizes the reverse argument, noting that poor health choices would likely exacerbate the risks of alcohol. “[A]lcohol would have a greater impact on the health of people who smoke, have poor diets, engage in low physical activity, are obese, have hepatitis infection, or have a family history of specific diseases than it would other individuals.”
Relative risks
In terms of relative risk of the range of conditions, generally, the ICCPUD study found small, if any, increases in risk at the three lowest levels of drinking, with risks rising with higher levels. The study’s finding of breast cancer risk was in line with the National Academies’ review. ICCPUD found that pre-menopausal females who drink moderately (one drink per day) had a 6 percent higher risk of breast cancer than non-drinkers, while post-menopausal moderate drinkers had a 17 percent higher risk. (You can see the complete set of relative risk estimates in Table A6 beginning on page 70 of the report.)
For some cancers, moderate drinking raised the risk substantially. For instance, males who have two drinks per day see their risk of esophageal cancer more than double. But, it’s important to note that the absolute risk for many of these cancers is small to begin with. The average risk of esophageal cancer in men is 0.8 percent, according to the American Cancer Society. With the increased risk from moderate drinking, it would be below 2 percent. Still, alcohol consumption increased the risks of nearly all the cancers examined, with the higher levels of alcohol consumption having the highest risk.
As for cardiovascular risks, ICCPUD’s review found low risk in several of the categories. The risk of ischemic heart disease was lower than that of nondrinkers at all six drinking levels. The risk of ischemic stroke was lower among drinkers who had one, two, three, or seven drinks per week compared to non-drinkers. At 14 and 21 drinks per week, the risk of ischemic stroke rose by 8 percent.
Beth is Ars Technica’s Senior Health Reporter. Beth has a Ph.D. in microbiology from the University of North Carolina at Chapel Hill and attended the Science Communication program at the University of California, Santa Cruz. She specializes in covering infectious diseases, public health, and microbes.
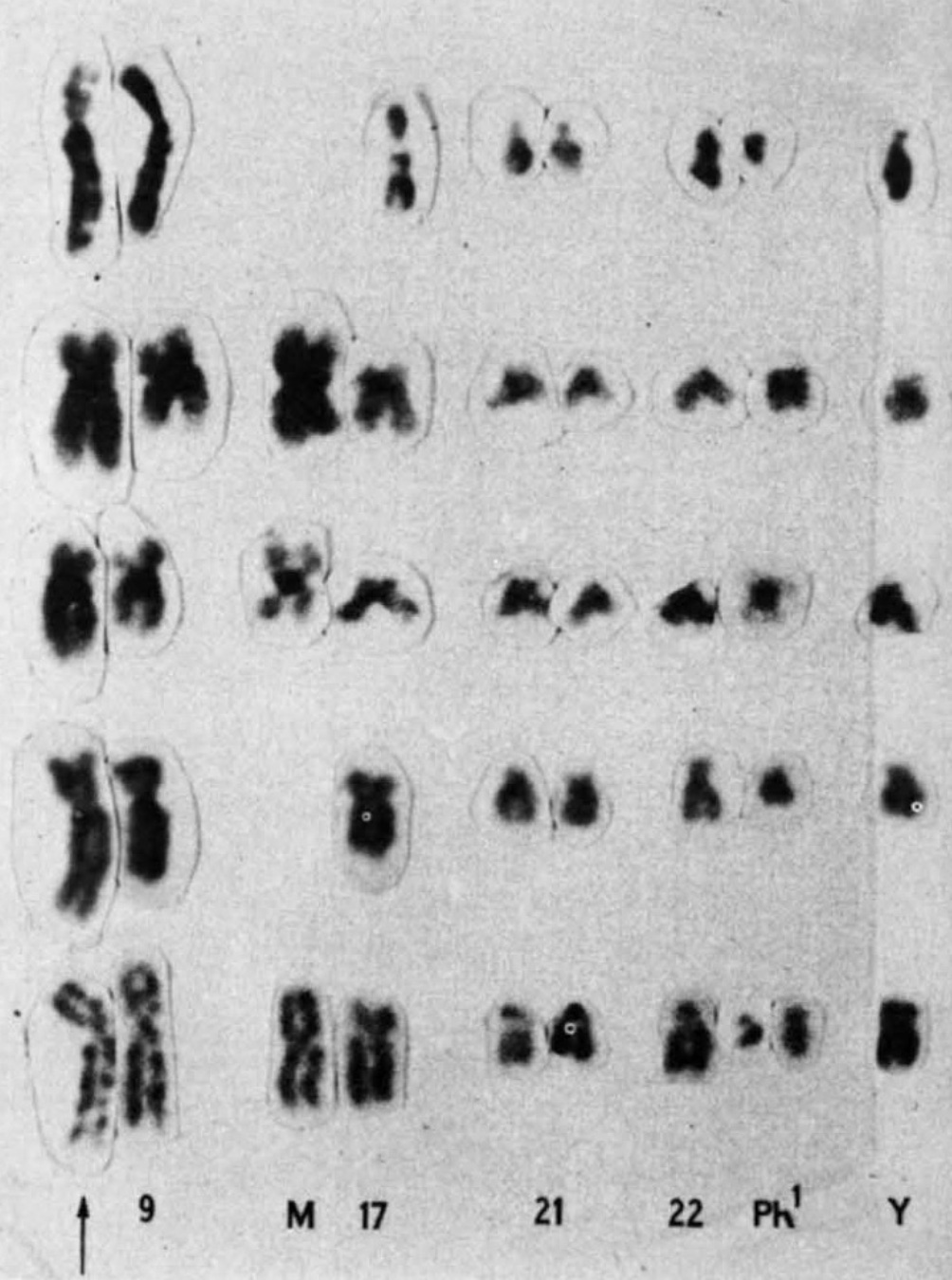
In 1972, Janet Rowley sat at her dining room table and cut tiny chromosomes from photographs she had taken in her laboratory. One by one, she snipped out the small figures her children teasingly called paper dolls. She then carefully laid them out in 23 matching pairs—and warned her kids not to sneeze.
The physician-scientist had just mastered a new chromosome-staining technique in a year-long sabbatical at Oxford. But it was in the dining room of her Chicago home where she made the discovery that would dramatically alter the course of cancer research.
Enlarge/ Rowley’s 1973 partial karyotype showing the 9;22 translocation
Looking over the chromosomes of a patient with acute myeloid leukemia (AML), she realized that segments of chromosomes 8 and 21 had broken off and swapped places—a genetic trade called a translocation. She looked at the chromosomes of other AML patients and saw the same switch: the 8;21 translocation.
Later that same year, she saw another translocation, this time in patients with a different type of blood cancer, called chronic myelogenous leukemia (CML). Patients with CML were known to carry a puzzling abnormality in chromosome 22 that made it appear shorter than normal. The abnormality was called the Philadelphia chromosome after its discovery by two researchers in Philadelphia in 1959. But it wasn’t until Rowley pored over her meticulously set dining table that it became clear why chromosome 22 was shorter—a chunk of it had broken off and traded places with a small section of chromosome 9, a 9;22 translocation.
Rowley had the first evidence that genetic abnormalities were the cause of cancer. She published her findings in 1973, with the CML translocation published in a single-author study in Nature. In the years that followed, she strongly advocated for the idea that the abnormalities were significant for cancer. But she was initially met with skepticism. At the time, many researchers considered chromosomal abnormalities to be a result of cancer, not the other way around. Rowley’s findings were rejected from the prestigious New England Journal of Medicine. “I got sort of amused tolerance at the beginning,” she said before her death in 2013.
The birth of targeted treatments
But the evidence mounted quickly. In 1977, Rowley and two of her colleagues at the University of Chicago identified another chromosomal translocation—15;17—that causes a rare blood cancer called acute promyelocytic leukemia. By 1990, over 70 translocations had been identified in cancers.
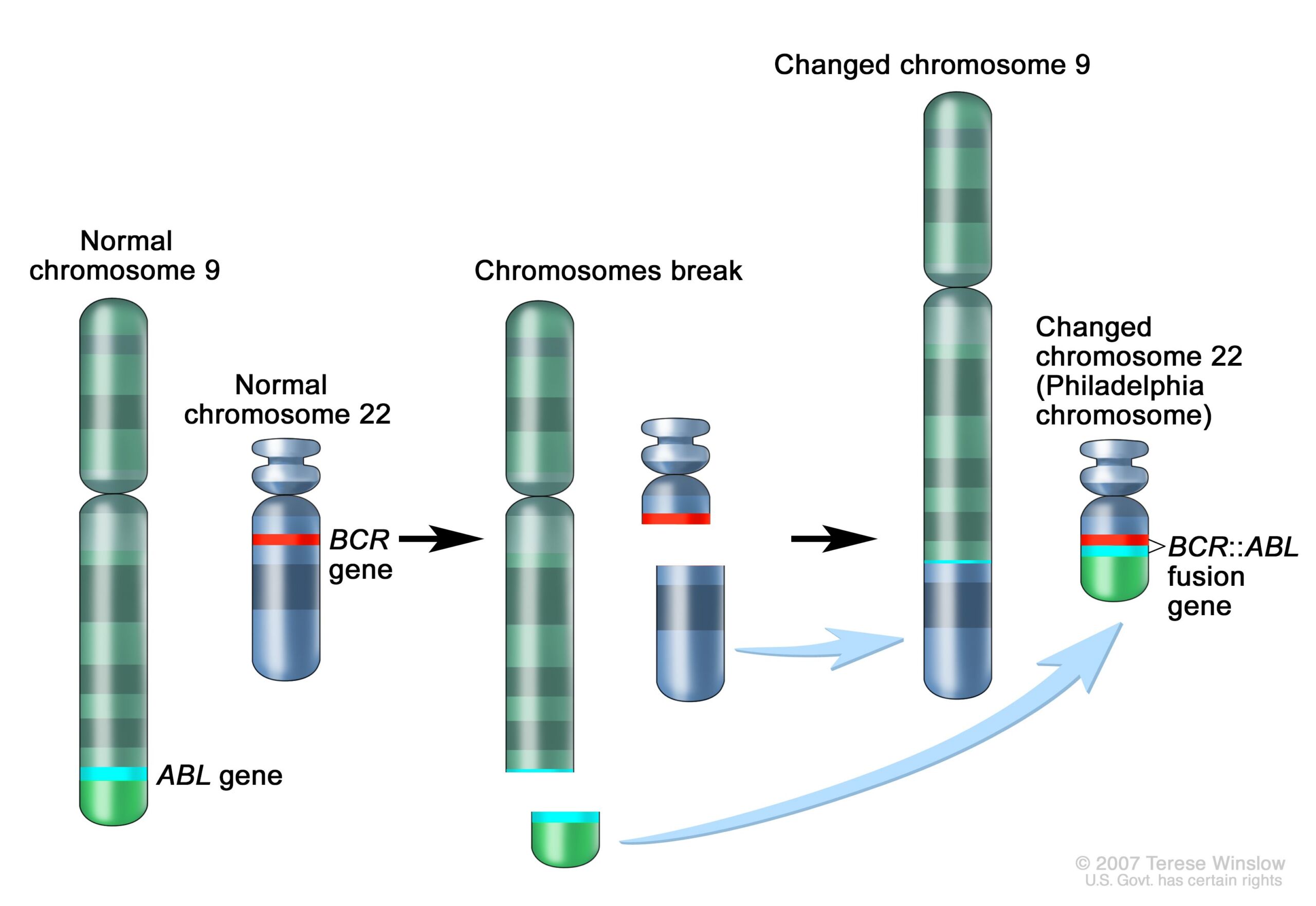
The significance mounted quickly as well. Following Rowley’s discovery of the 9;22 translocation in CML, researchers figured out that the genetic swap creates a fusion of two genes. Part of the ABL gene normally found on chromosome 9 becomes attached to the BCR gene on chromosome 22, creating the cancer-driving BCR::ABL fusion gene on chromosome 22. This genetic merger codes for a signaling protein—a tyrosine kinase—that is permanently stuck in “active” mode. As such, it perpetually triggers signaling pathways that lead white blood cells to grow uncontrollably.
Enlarge/ Schematic of the 9;22 translocation and the creation of the BCR::ABL fusion gene.
By the mid-1990s, researchers had developed a drug that blocks the BCR-ABL protein, a tyrosine kinase inhibitor (TKI) called imatinib. For patients in the chronic phase of CML—about 90 percent of CML patients—imatinib raised the 10-year survival rate from less than 50 percent to a little over 80 percent. Imatinib (sold as Gleevec or Glivec) earned approval from the Food and Drug Administration in 2001, marking the first approval for a cancer therapy targeting a known genetic alteration.
With imatinib’s success, targeted cancer therapies—aka precision medicine—took off. By the early 2000s, there was widespread interest among researchers to precisely identify the genetic underpinnings of cancer. At the same time, the revolutionary development of next-generation genetic sequencing acted like jet fuel for the soaring field. The technology eased the identification of mutations and genetic abnormalities driving cancers. Sequencing is now considered standard care in the diagnosis, treatment, and management of many cancers.
The development of gene-targeting cancer therapies skyrocketed. Classes of TKIs, like imatinib, expanded particularly fast. There are now over 50 FDA-approved TKIs targeting a wide variety of cancers. For instance, the TKIs lapatinib, neratinib, tucatinib, and pyrotinib target human epidermal growth factor receptor 2 (HER2), which runs amok in some breast and gastric cancers. The TKI ruxolitinib targets Janus kinase 2, which is often mutated in the rare blood cancer myelofibrosis and the slow-growing blood cancer polycythemia vera. CML patients, meanwhile, now have five TKI therapies to choose from.
Enlarge/ Ozempic is a GLP-1 drug for adults with type 2 diabetes.
For patients with Type 2 diabetes, taking one of the new GLP-1 drugs, such as Ozempic, is associated with lower risks of developing 10 out of 13 obesity-associated cancers as compared with taking insulin, according to a recent study published in JAMA Network Open.
The study was retrospective, capturing data from over 1.6 million patients with Type 2 diabetes but no history of obesity-associated cancers prior to the study period. Using electronic health records, researchers had follow-up data for up to 15 years after the patients started taking either a GLP-1 drug, insulin, or metformin between 2008 and 2015.
This type of study can’t prove that the GLP-1 drugs caused the lower associated risks, but the results fit with some earlier findings. That includes results from one trial that found a 32 percent overall lower risk of obesity-associated cancers following bariatric surgery for weight loss.
In the new study, led by researchers at Case Western Reserve University School of Medicine, some of the GLP-1-associated risk reductions were quite substantial. Compared with patients taking insulin, patients taking a GLP-1 drug had a 65 percent lower associated risk of gall bladder cancer, a 63 percent lower associated risk of meningioma (a type of brain tumor), a 59 percent lower associated risk for pancreatic cancer, and a 53 percent lower associated risk of hepatocellular carcinoma (liver cancer). The researchers also found lower associated risks for esophageal cancer, colorectal cancer, kidney cancer, ovarian cancer, endometrial cancer, and multiple myeloma.
Compared with insulin, the researchers saw no lowered associated risk for thyroid and breast cancers. There was a lower risk of stomach cancer calculated, but the finding was not statistically significant.
Gaps and goals
The GLP-1 drugs did not show such promising results against metformin in the study. Compared with patients taking metformin, patients on GLP-1 drugs saw lower associated risks of colorectal cancer, gall bladder cancer, and meningioma, but those calculations were not statistically significant. The results also unexpectedly indicated a higher risk of kidney cancer for those taking GLP-1 drugs, but the cause of that potentially higher risk (which was not seen in the comparison with insulins) is unclear. The researchers called for more research to investigate that possible association.
Overall, the researchers call for far more studies to try to confirm a link between GLP-1 drugs and lower cancer risks, as well as studies to try to understand the mechanisms behind those potential risk reductions. It’s unclear if the lower risks may be driven simply by weight loss, or if insulin resistance, blood sugar levels, or some other mechanisms are at play.
The current study had several limitations given its retrospective, records-based design. Perhaps the biggest one is that the data didn’t allow the researchers to track individual patients’ weights throughout the study period. As such, researchers couldn’t examine associated cancer risk reductions with actual weight loss. It’s one more aspect that warrants further research.
Still, the study provides another promising result for the blockbuster, albeit pricy, drugs. The researchers suggest extending their work to assess whether GLP-1 drugs could be used to improve outcomes in patients with Type 2 diabetes or obesity who are already diagnosed with cancer, in addition to understanding if the drugs can help prevent the cancer.
Enlarge/ Pharma interest and investment in radiotherapy drugs is heating up.
Knowable Magazine
On a Wednesday morning in late January 1896 at a small light bulb factory in Chicago, a middle-aged woman named Rose Lee found herself at the heart of a groundbreaking medical endeavor. With an X-ray tube positioned above the tumor in her left breast, Lee was treated with a torrent of high-energy particles that penetrated into the malignant mass.
“And so,” as her treating clinician later wrote, “without the blaring of trumpets or the beating of drums, X-ray therapy was born.”
Radiation therapy has come a long way since those early beginnings. The discovery of radium and other radioactive metals opened the doors to administering higher doses of radiation to target cancers located deeper within the body. The introduction of proton therapy later made it possible to precisely guide radiation beams to tumors, thus reducing damage to surrounding healthy tissues—a degree of accuracy that was further refined through improvements in medical physics, computer technologies and state-of-the-art imaging techniques.
But it wasn’t until the new millennium, with the arrival of targeted radiopharmaceuticals, that the field achieved a new level of molecular precision. These agents, akin to heat-seeking missiles programmed to hunt down cancer, journey through the bloodstream to deliver their radioactive warheads directly at the tumor site.
Use of radiation to kill cancer cells has a long history. In this 1915 photo, a woman receives “roentgenotherapy”—treatment with X-rays—directed at an epithelial-cell cancer on her face.
Wikimedia Commons
Today, only a handful of these therapies are commercially available for patients—specifically, for forms of prostate cancer and for tumors originating within hormone-producing cells of the pancreas and gastrointestinal tract. But this number is poised to grow as major players in the biopharmaceutical industry begin to invest heavily in the technology.
AstraZeneca became the latest heavyweight to join the field when, on June 4, the company completed its purchase of Fusion Pharmaceuticals, maker of next-generation radiopharmaceuticals, in a deal worth up to $2.4 billion. The move follows similar billion-dollar-plus transactions made in recent months by Bristol Myers Squibb (BMS) and Eli Lilly, along with earlier takeovers of innovative radiopharmaceutical firms by Novartis, which continued its acquisition streak—begun in 2018—with another planned $1 billion upfront payment for a radiopharma startup, as revealed in May.
“It’s incredible how, suddenly, it’s all the rage,” says George Sgouros, a radiological physicist at Johns Hopkins University School of Medicine in Baltimore and the founder of Rapid, a Baltimore-based company that provides software and imaging services to support radiopharmaceutical drug development. This surge in interest, he points out, underscores a wider recognition that radiopharmaceuticals offer “a fundamentally different way of treating cancer.”
Treating cancer differently, however, means navigating a minefield of unique challenges, particularly in the manufacturing and meticulously timed distribution of these new therapies, before the radioactivity decays. Expanding the reach of the therapy to treat a broader array of cancers will also require harnessing new kinds of tumor-killing particles and finding additional suitable targets.
“There’s a lot of potential here,” says David Nierengarten, an analyst who covers the radiopharmaceutical space for Wedbush Securities in San Francisco. But, he adds, “There’s still a lot of room for improvement.”
Atomic advances
For decades, a radioactive form of iodine stood as the sole radiopharmaceutical available on the market. Once ingested, this iodine gets taken up by the thyroid, where it helps to destroy cancerous cells of that butterfly-shaped gland in the neck—a treatment technique established in the 1940s that remains in common use today.
But the targeted nature of this strategy is not widely applicable to other tumor types.
The thyroid is naturally inclined to absorb iodine from the bloodstream since this mineral, which is found in its nonradioactive form in many foods, is required for the synthesis of certain hormones made by the gland.
Other cancers don’t have a comparable affinity for radioactive elements. So instead of hijacking natural physiological pathways, researchers have had to design drugs that are capable of recognizing and latching onto specific proteins made by tumor cells. These drugs are then further engineered to act as targeted carriers, delivering radioactive isotopes—unstable atoms that emit nuclear energy—straight to the malignant site.
The North Carolina State Senate on Wednesday voted 30–15, along party lines, in favor of a Republican bill that would make it illegal for people in the state to wear a mask in public for health reasons. The bill is now moving to the House, where it could potentially see changes.
The proposed ban on health-based masking is part of a larger bill otherwise aimed at increasing penalties for people wearing masks to conceal their identity while committing a crime or impeding traffic. The bill was largely spurred by recent protests on university and college campuses across the country, including North Carolina-based schools, against the war in Gaza. In recent months, there have been demonstrations in Raleigh and Durham that have blocked roadways, as well as clashes on the nearby campus of the University of North Carolina at Chapel Hill. Some demonstrators were seen wearing masks in those events.
But the bill, House Bill 237, goes a step further by making it illegal to wear a mask in public for health and safety reasons, either to protect the wearer, those around them, or both. Specifically, the bill repeals a 2020 legal exemption enacted amid the COVID-19 pandemic, which allowed for public health-based masking for the first time in decades.
Prior to 2020, laws dating back to 1953 largely prohibited public masking. The prohibition was part of a crackdown on “secret societies” at the time, or more specifically, an attempt to curtail the activities of the Ku Klux Clan in the state. Exemptions only existed for things like holiday costumes, theater productions, gas masks, and members of public parades or ceremonies that had obtained permits.
On Wednesday, North Carolina residents with compromised immune systems spoke—while masked—during a public comment section. Simone Hetherington told lawmakers that masking was the only way to protect herself in public from illness and feared passage of the bill would prevent her from doing so, according to reporting by the Associated Press.
But, according to The News & Observer, Republicans were dismissive of that possibility, arguing that in the decades prior to the pandemic, when public masking was largely illegal, they couldn’t recall anyone being prosecuted for wearing a mask for health reasons.
Raleigh-based news outlet WRAL quoted Sen. Sydney Batch, a Democrat from Wake, who criticized the bill along with fellow Democratic colleagues. Batch, a cancer survivor, spoke of how her husband and children wore masks to protect her while she underwent cancer treatments that weakened her immune system. “This bill criminalizes their behavior and mine,” she said. “We talk a lot about freedoms in this chamber. I hear it all the time. I should have the freedom—my children and my husband should have the freedom—to wear masks in order to protect and save my life, without fear of being arrested and charged.”












{kind=link}
{kind=link}